
Low-GI diets help most in metabolic disease
A June 2026 meta-analysis in Frontiers in Nutrition pooled 21 RCTs (n=1,265) on low-glycemic-index/load diets and found large pooled SMDs for weight, lipids, and CRP — but I² values of 88–95% make the numbers clinically uninterpretable as individual predictions. The critical subgroup finding: LDL-C benefits concentrate entirely in people with existing metabolic disease (SMD −1.85, p=0.03), while metabolically healthy adults show essentially no effect (SMD −0.07, p=0.62). TNF-α and IL-6 are statistically fragile (each loses significance when one trial is removed). Actionable takeaway: the whole-grain/legume swap is well-evidenced for patients managing T2DM, metabolic syndrome, or obesity; healthy adults have no strong metabolic rationale from this study.

Vistazo a la investigación
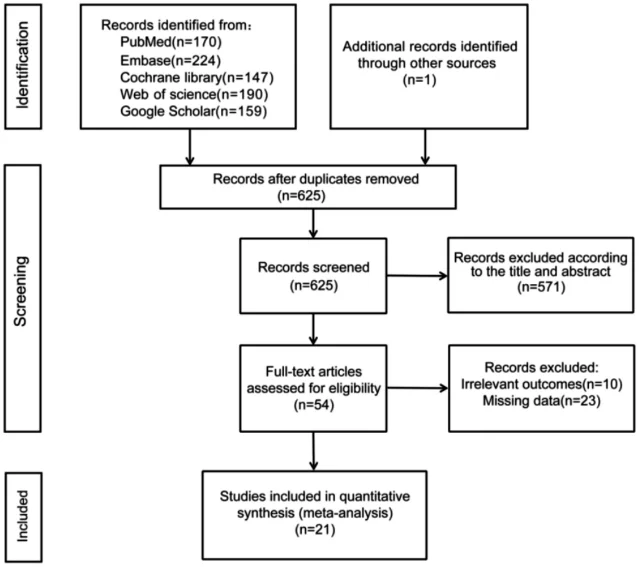
What the researchers did
The outcomes that held up
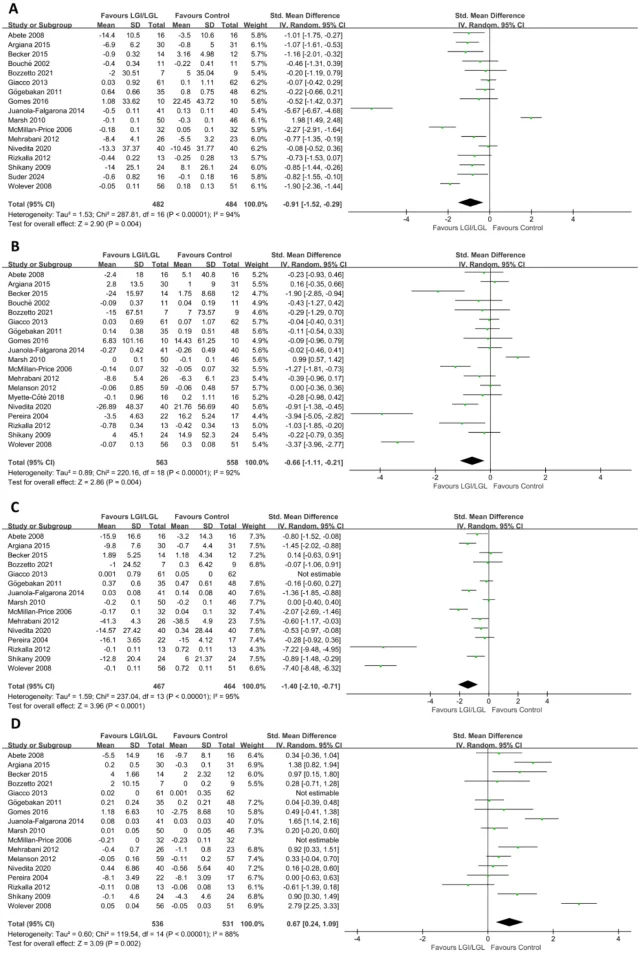
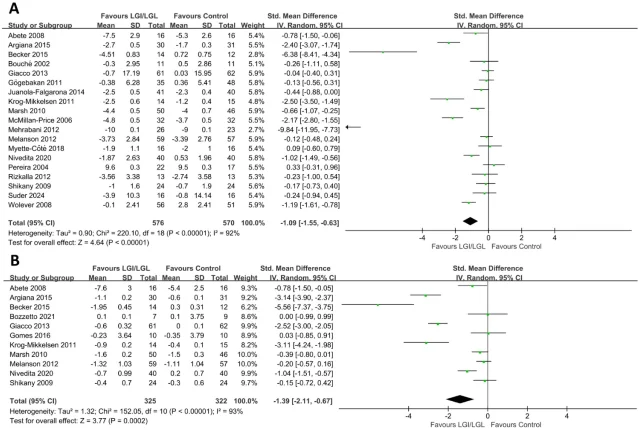
| Outcome | Trials (n) | Pooled SMD (95% CI) | p-value | I² |
|---|---|---|---|---|
| Body weight | 19 | −1.09 (−1.55, −0.63) | <0.001 | 92% |
| BMI | 11 | −1.39 (−2.11, −0.67) | <0.001 | 93% |
| LDL-C | 15 | −1.40 (−2.10, −0.71) | <0.001 | 95% |
| Triglycerides | 19 | −0.66 (−1.11, −0.21) | 0.004 | 92% |
| Total cholesterol | 17 | −0.91 (−1.52, −0.29) | 0.004 | 94% |
| HDL-C | 17 | +0.67 (+0.24, +1.09) | 0.004 | 88% |
| CRP | 14 | −0.86 (−1.30, −0.41) | <0.001 | 91% |
| Leptin | 10 | −1.11 (−1.81, −0.40) | 0.002 | 90% |
The outcomes that did not hold up
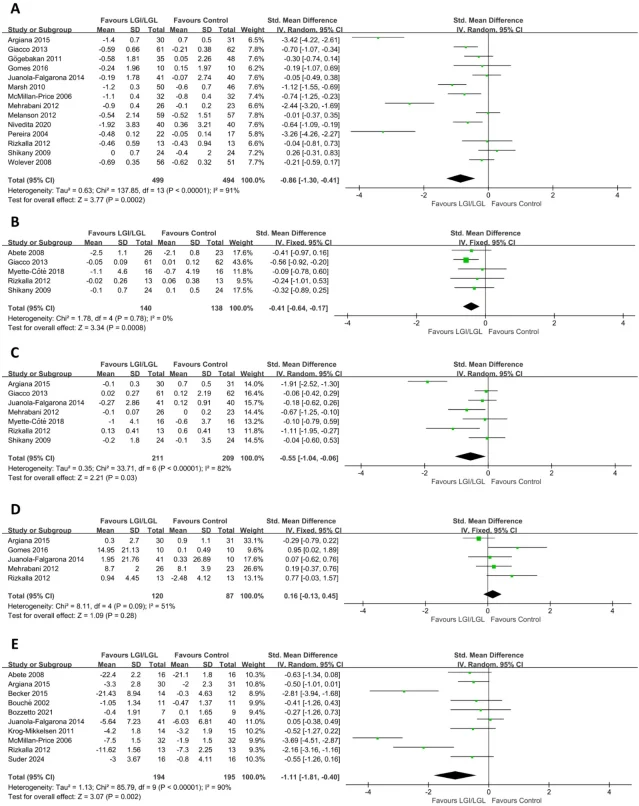
The finding that matters most: who benefits for LDL-C
| Health status subgroup | Trials | SMD (95% CI) | p-value |
|---|---|---|---|
| Metabolic conditions (T2DM, MS) | 5 | −1.85 (−3.51, −0.19) | 0.03 |
| Overweight/obese | 8 | −1.22 (−1.91, −0.52) | <0.001 |
| Healthy individuals | 2 | −0.07 (−0.37, 0.22) | 0.62 |
Limitations
What to do with this today
- Replace white rice and white bread with intact whole grains (barley, bulgur, oats, whole-grain rye bread). GI drops from ~70–85 to ~40–55.
- Replace sugary breakfast cereals with rolled oats or steel-cut oats. GI drops from ~80 to ~55.
- Add lentils, chickpeas, or kidney beans to one or two meals per week. Most legumes have GI values below 40.
- Choose whole fruit over fruit juice; the intact fiber matrix slows glucose absorption.
Añade más opiniones o contexto en torno a este contenido.